The sterile environment of a hospital room transformed into an unexpected courtroom for Cherise Doyley, a pregnant mother of three, as she found herself defending her birth plan to a judge via a video call while in active labor at the University of Florida Health hospital in downtown Jacksonville. This extraordinary event, captured on video, has ignited a national conversation about bodily autonomy, medical ethics, and the escalating impact of "fetal personhood" policies on pregnant individuals in the United States. Doyley’s ordeal serves as a stark illustration of how constitutional rights can seemingly diminish when a woman becomes pregnant, forcing her to contend with legal mandates over her own medical decisions.
A Planned Birth Derailed by Legal Intervention
Cherise Doyley, experienced in the intricacies of childbirth not only as a mother but also as a professional birthing doula, arrived at UF Health Jacksonville with a clear intention: to attempt a vaginal delivery. Her background provided her with a nuanced understanding that while birth plans are essential, flexibility is equally crucial. However, she was firm in her desire to avoid a repeat cesarean section if a vaginal birth after cesarean (VBAC) was medically viable.
Her labor began overnight after her water broke. Upon admission, doctors expressed concerns about the risk of uterine rupture, a potentially life-threatening complication for both mother and baby, especially in cases of VBAC. Doyley, informed by her extensive knowledge, understood the presented risk to be less than 2%. She consistently communicated her non-consent to an immediate C-section without first attempting a vaginal delivery, a decision rooted in her informed assessment of the risks and benefits. Initially, medical staff appeared to accommodate her wishes, allowing her to continue laboring for several hours.
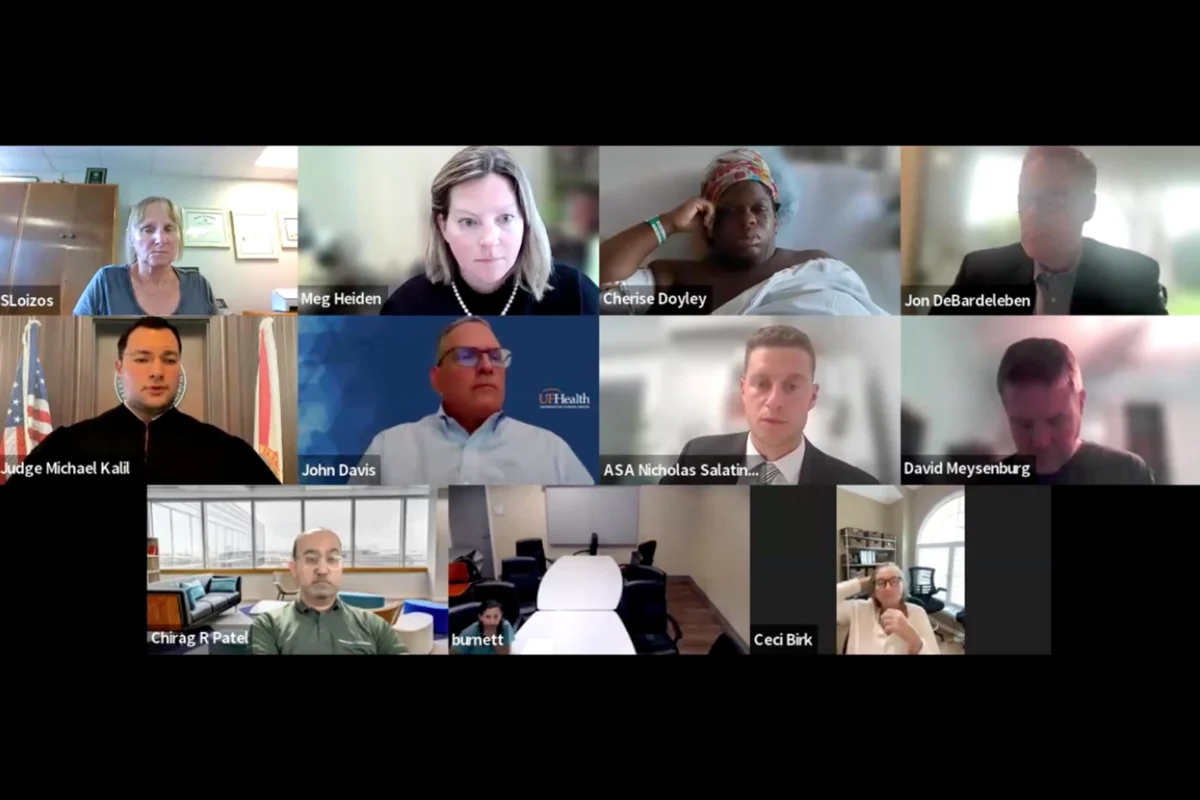
The situation took a bewildering turn when a nursing supervisor approached Doyley’s bedside, not with an update on her labor progression, but with a tablet. The shocking revelation that she was in court, facing legal action for declining a C-section, marked an unprecedented intrusion into one of life’s most personal and vulnerable moments. The confusion and disbelief on Doyley’s face, captured in the video recording obtained by ProPublica, underscored the profound violation of her autonomy.
Fetal Personhood and the Erosion of Rights
This incident is not an isolated anomaly but rather a symptom of a broader legal and societal shift, particularly in states like Florida that have embraced "fetal personhood" policies. These policies, which grant fetuses legal status akin to children, are increasingly shaping healthcare decisions and challenging established principles of bodily autonomy. For decades, legal precedents have affirmed an individual’s right to refuse medical treatment, even if such refusal could be life-saving for themselves or others. Yet, as Doyley’s case painfully demonstrates, pregnant women frequently find themselves to be a rare exception to this fundamental right.
The reporter, based in Alabama, noted how this philosophy mirrors the legal challenges faced by women in states with strict fetal personhood policies. Investigations have revealed eerily similar scenarios involving women like Brianna Bennett in Florida, who also found themselves battling in court for their right to make medical decisions during pregnancy. This emerging trend raises critical questions about who ultimately controls a pregnant woman’s body and medical care. In several states, judges have intervened to mandate blood transfusions, enforce bed rest, or, as in Doyley’s situation, compel major surgery, all purportedly in the "best interest" of the fetus.
Medical Arguments and Conflicting Perspectives
During the virtual hearing, which lasted over two hours, a panel of medical and legal professionals, predominantly white, surrounded Doyley on the screen as she lay in her hospital bed, hooked up to IVs and monitors. Judge Michael Kalil presided, explaining the proceedings initiated by the State Attorney’s office at the hospital’s request to grant an emergency C-section order.
Dr. Erin Burnett, one of the physicians involved, testified that she believed Doyley could not achieve a successful vaginal birth and that prolonged labor would significantly increase the risk of uterine rupture, endangering both Doyley and the baby. Dr. John Davis, chair of the obstetrics and gynecology department, further asserted the hospital’s reputation for a low C-section rate, implying that their recommendation for intervention was solely medically driven. Jenny Van Ravestein, director of women’s services, reiterated the collective concern for the baby’s welfare. However, both Burnett and Davis declined subsequent requests for comment, and the hospital cited patient privacy in refusing interviews with its staff.
The medical literature regarding the risks of uterine rupture after prior C-sections is complex and often subject to interpretation. Studies indicate a rupture risk ranging from 0.15% to 2.3%, influenced by factors such as body mass index, prior successful vaginal births, and whether labor is spontaneous or induced. For Doyley, these percentages, even at their higher end, felt sufficiently low to warrant attempting a VBAC. Crucially, the medical testimony presented during the hearing largely omitted a comprehensive discussion of the significant downsides and potential complications associated with a repeat C-section for Doyley herself. These include a longer, more arduous recovery, increased risk of infection, future pregnancy complications, and, albeit rare, the risk of maternal mortality.
Doyley’s Plea: Risks to Herself and Her Family
Initially muted, Doyley was eventually granted the opportunity to testify. Her reasons for wanting to avoid another major abdominal surgery were deeply personal and critically important. She had endured difficult recoveries from her previous C-sections, including a severe hemorrhage after one delivery that necessitated a week-long re-hospitalization. The prospect of another complicated recovery filled her with dread, as it would severely impair her ability to care for her three existing children. Her deepest fear was the catastrophic scenario of her own death, which could leave her children vulnerable to entering the foster care system. For Doyley, a C-section was far from a "low-risk" option; it presented substantial, personal risks to her life and the stability of her family.
During her testimony, Doyley poignantly questioned whether her life and the lives of her other children mattered to the hospital and the medical team. Kimberly Mutcherson, a law professor at Rutgers University, commented on how women who challenge medical advice often face accusations of maternal neglect. "You’re somebody who is a bad mother, right?" Mutcherson articulated, highlighting the societal expectation that mothers must sacrifice, even their bodily autonomy, for their children. Elizabeth Kukura, a law professor at Drexel University, added that such interventions reflect a troubling perception of women primarily as "incubators" or "childbearers," rather than individuals with inherent rights and complex needs.
The Ethical Quandary in Obstetrics
The ethical guidelines of the American College of Obstetricians and Gynecologists (ACOG) stipulate that when the needs of the mother and fetus conflict, the physician’s primary responsibility is to the well-being of the mother. This principle acknowledges the mother as the primary patient whose autonomy and health are paramount. However, cases like Doyley’s illustrate a concerning deviation, where the perceived welfare of the fetus is elevated above the informed consent and bodily integrity of the pregnant woman. This creates a dangerous precedent that undermines the foundational trust in the doctor-patient relationship and challenges established medical ethics.
A Scene of Disparity and a Forced Outcome
The virtual hearing itself was a stark visual representation of the power imbalance. Doyley, a Black woman, vulnerable in a hospital bed, faced a cadre of mostly white medical and legal professionals. She requested legal counsel or at least a patient advocate, but Florida courts do not mandate such provisions for pregnant women in these hearings, leaving her to navigate the complex legal arguments alone. The experience was not just legally challenging but deeply isolating and disempowering.
Expressing a profound lack of trust, Doyley asked for a transfer to another hospital, unwilling to have anyone involved in the hearing perform her C-section. Hospital officials deemed this unlikely, as another facility would first have to accept her. She then requested that Black nurses or doctors be assigned to her care, raising unspoken concerns about racial bias within the healthcare system. Her desperate question — "They’re going to tie me up and go give me a C-section against my will?" — underscored her terror of forced medical intervention.
Ultimately, Judge Kalil did not order an immediate C-section but issued a ruling that permitted the hospital to perform one in an emergency without Doyley’s explicit consent, setting a 6 a.m. deadline for further assessment. Doyley, maintaining remarkable composure under immense duress, ended the hearing with a pointed, sarcastic thank you to the judge: "I appreciate you spending two hours on a Sunday going through my medical history and fighting for my vagina and my baby."
Emergency Intervention and Post-Surgical Hearing
In the early hours of the morning, hours after the judge’s ruling, Doyley’s fears materialized. Doctors reported a sustained drop in the baby’s heart rate, a medical emergency that led to Doyley being rushed into surgery. She gave birth to her daughter via C-section, a procedure she had fought so hard to avoid.
The ordeal, however, was far from over. Just two hours after her C-section, at 8 a.m., nurses again brought a tablet to her bedside for a final hearing. Exhausted, recovering from major surgery, and yet to see her newborn daughter who was in the neonatal intensive care unit, Doyley vehemently refused to participate. "Tell them I don’t want to be on," she stated. "Y’all can have your own meeting. I want to see my child." Upon hearing that the baby had been born, Judge Kalil closed the case, wishing Doyley well. The swift termination of the legal proceedings after the birth of the child further emphasized the singular focus on the fetus, seemingly at the expense of the mother’s immediate post-operative needs and desire to bond with her infant.
Institutional Silence and Lasting Trauma
In response to inquiries, Judge Kalil cited the judicial code of conduct, which prohibits judges from commenting on cases to preserve the integrity and neutrality of the judicial process. University of Florida Health in Jacksonville, despite Doyley signing a waiver allowing discussion of her case, also declined to comment, citing patient privacy. This institutional silence leaves many questions unanswered about the hospital’s protocol, the specific triggers for seeking a court order, and the ethical considerations involved.
For a year following the birth, Doyley and her family attempted to move past the traumatic experience. However, the profound feeling of violation lingered. She articulated a chilling warning: if the hospital could legally compel her to undergo surgery, it could happen to anyone. "When we use the courts to basically strong-arm, bully someone into an unnecessary medical procedure against their will, it’s akin to torture, in my eyes," Doyley powerfully concluded.
Broader Implications: A Chilling Precedent
Cherise Doyley’s case is more than an individual tragedy; it serves as a critical marker in the ongoing national debate surrounding reproductive rights, patient autonomy, and the increasing legal and medical scrutiny placed upon pregnant individuals.
-
Erosion of Informed Consent and Bodily Autonomy: The most immediate implication is the severe undermining of the principle of informed consent. If a patient, even one with extensive medical knowledge and a clear understanding of risks, can be legally compelled to undergo surgery against their will, the very foundation of patient-centered care is compromised. This sets a dangerous precedent for all medical decisions, especially for vulnerable populations.
-
Impact of Fetal Personhood Policies: The case vividly illustrates the real-world consequences of "fetal personhood" laws. While proponents argue these laws protect unborn life, critics contend they often come at the expense of a pregnant woman’s fundamental rights, transforming her into a mere vessel whose body can be legally commandeered. Florida’s aggressive stance on such policies suggests that more cases of forced medical intervention could emerge.
-
Healthcare Disparities and Racial Bias: Doyley, a Black woman, found herself in a situation where her medical judgment was questioned and ultimately overridden by a predominantly white medical and legal establishment. Her request for a Black care provider highlights a broader concern about racial disparities in maternal healthcare. Black women in the U.S. face significantly higher rates of maternal mortality and are often subjected to implicit bias and a lack of trust from medical professionals. Cases of forced interventions may disproportionately affect women of color, exacerbating existing inequalities.
-
Breakdown of Doctor-Patient Trust: When legal systems override medical ethics and patient autonomy, it inevitably erodes the trust essential to the doctor-patient relationship. Patients may become hesitant to seek care, fearing that their choices will be challenged or legally mandated, leading to potentially poorer health outcomes.
-
Legal and Ethical Quandaries for Medical Professionals: The case also places medical professionals in an unenviable position, caught between their professional obligation to patients, institutional pressures, and legal mandates. It forces a re-evaluation of ethical guidelines and the potential need for clearer legal protections for both patients and healthcare providers.
Cherise Doyley’s harrowing experience in a Jacksonville hospital room underscores a growing crisis at the intersection of law, medicine, and personal liberty. Her fight for her birth plan, while in labor, serves as a poignant warning about the future of reproductive autonomy and the urgent need to safeguard the rights of pregnant individuals in an evolving legal landscape.